










Avian pneumovirus, current status and control programmes used
Since it was identified by Buys & Du Preez in 1978 as the causal agent of turkey rhinotracheitis, avian pneumovirus or avian metapneumovirus (aMPV) has been associated with clinical symptoms in different countries, and subsequently also in broilers, layers and breeders as the agent that causes Swollen Head Syndrome (SHS). This situation is the direct result of better laboratory diagnosis in suspicious clinical cases, and of growing interest due to losses. 24 January 2018
24 January 2018
 8 minute read
8 minute read
 by Javier Sanz Corella, DVM Corporate Group Product Manager, Poultry Business Unit Hipra. Spain
by Javier Sanz Corella, DVM Corporate Group Product Manager, Poultry Business Unit Hipra. Spain
Avian metapneumovirus is replicated in the upper respiratory tract in chickens of any age from birth (Hafez 1993; Cook 2000) and in the reproductive tract after a viraemic phase.
Seroprevalence is high in breeders, although not always accompanied by clinical symptoms in broilers (O’Brien 1985; Hafez and Löhren 1990; Owoade et al. 2006).
It is replicated in ciliated epithelial cells in the nasal turbinates and trachea, causing ciliate deformity and loss in these areas, facilitating access for secondary agents (Majó et al. 1996) that complicate and aggravate the pathological process.
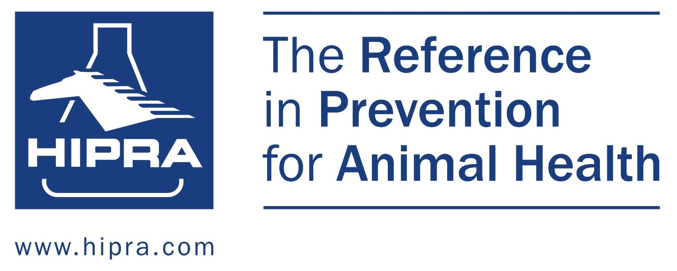
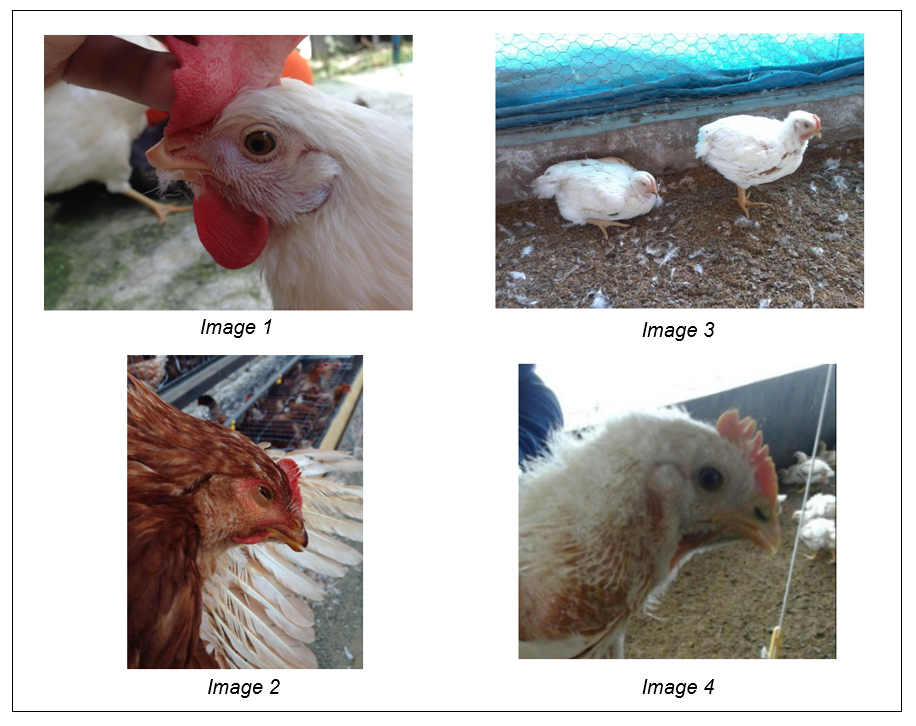
Clinical signs are largely respiratory, including sneezing, coughing, nasal secretion, conjunctivitis and oedematous sinuses (Images 1 and 2), and swollen head can present in complex cases with bacterial infections (Images 3 and 4). The infection caused by aMPV favours the onset of secondary respiratory infections in chickens and turkeys, as shown with several respiratory pathogens (Naylor et al., 1992; Van de Zande et al., 2001; Marien et al., 2005; Van Loock et al., 2006).
Breeders and layers are also prone to viral replication in the oviduct, with drop in egg production, and affecting egg shell quality. Other symptoms are nervousness, torticollis and opisthotonus, due to ascending bacterial infections from the middle ear, which cause cranial osteomyelitis (Majó et al. 1996).
In laying hensl, productive stress triggers the onset of most clinical cases in both layers and breeders.
Clinical diagnosis is not 100% reliable, and can only be used as a guide for definitive diagnosis. Diagnosis ultimately depends on the interpretation of laboratory tests, largely serology (ELISA), confirmed in unclear cases by PCR, although it is difficult due to the short period in which the virus can be found in the target tissues and the few symptoms found at the time (Baxter-Jones & Jones, 1989; Alexander 1991; Majó et al. 1995), although it can be detected up to 17 days post-inoculation in laboratory conditions (Jing et al. 1993).
Vaccination programmes used
There are currently different vaccination programmes, depending on the status of the disease in each country and different epidemiological situations. Countries can be classified as: with no registered vaccines, only registered inactivated vaccines, or countries with live and inactivated vaccines.
And then we have to consider the type of bird to be vaccinated against aMPV. In general, long cycle birds will receive live and inactivated vaccines (if they are permitted), while short cycle or meat production poultry only receive live vaccines.
To maximise the efficacy of aMPV vaccination programmes, our recommendations are based on several common factors applicable to all situations:
- Always start vaccination programmes prior to contact with the field virus . Using ELISA results at different ages.
- Apply live vaccines directly to the target tissue (upper respiratory tract) by coarse spray or eye drop vaccination.
- To programme vaccination ages, applications between live vaccines and between live and inactivated vaccines should be no more than 6 weeks apart.
Short cycle or meat production poultry
Vaccination is a preventive tool in meat producers; vaccination can be seasonal during the time of the year when there are most problems, or continuous in areas with high viral circulation. The challenge can be easily evaluated by ELISA at slaughter age.
Several authors have shown that live vaccines are effective, irrespective of the seroconversion produced (Cook et al. 1989; Williams et al. 1991; Ganapathy & Jones, 2007; S. Corella et al. 2015) as immunity is mainly local (Cook et al. 1989; Williams et al. 1991; Jones et al. 1992).
Live vaccines such as HIPRAVIAR® SHS can be used in the control of aMPV in broiler chickens, while evaluating the extent to which viral circulation is limited, as the serological results will tell us whether the virus continues to circulate or has been reduced or disappeared. According to these results, the vaccination programme can be switched from seasonal to continuous, or vice versa.
In broiler turkeys, 2 to 3 doses would be applied, depending on growing management. Turkeys are much more prone to the virus, so much shorter periods between live vaccines (10 to 21 days) are not used.
Long cycle poultry or layers
In layers, aMPV is a long-term challenge for health and, thus, for economic returns. The disease presents clinical symptoms largely in the production phase, so corrective measures are difficult, if not impossible, at this time. There is an increase in the incidence of bacterial problems, with the necessary antibiotic treatment, and a drop in production or quality, with a negative impact on returns.
There are 2 types of vaccination programmes for layers, determined by the registration of live or inactivated vaccines:
Countries where only inactivated vaccines can be used
In countries that only permit inactivated vaccines, vaccination programmes depend on epidemiology in each region. The most common programme comprises 2 doses of inactivated vaccine, the first before the first contact with the field virus with the second being 2 to 3 weeks before the pullets are transferred to production farms.
The greatest challenge in these countries is to design the most appropriate vaccination plan. In our experience, future layers and breeders come into contact with aMPV from 6 to 12 weeks of age, depending on the region, although in some cases initial contact is much earlier, at around 3 weeks of age.
Thanks to the analysis of more than 1000 blood samples in Colombia, using a programme of 2 doses of HIPRAVIAR® TRT (inactivated vaccine) (G2) versus one (G1) or no doses (G0), HIPRAVIAR® TRT reduced the circulation of field viruses in vaccinated farms, as shown on Figure 1, when comparing antibody levels between hens from different farms (S. Corella et al. 2017).
.PNG)
Figure 1. Mean aMPV antibody titre in different study groups and different age ranges. Different superscripts show significant differences using the Mann-Whitney U-test with p-value <0.05.
* Weeks
Inactivated vaccines are very important for long cycle poultry, and are the only control method in situations where live vaccines are not allowed. The main functions of inactivated vaccines are:
- Reduction in field virus excretion in the event of infection (Cook et al, 1989; Hess et al, 2004)
- Reduction in severity of respiratory symptoms in the event of infection
- Prevention of field virus replication in the reproductive tract, protecting egg production and egg shell quality.
Countries where live and inactivated vaccines are allowed
The most common vaccination programmes, depending on the country and epidemiology, are:
- 2 to 3 doses of live vaccine, plus one dose of inactivated vaccine before transfer to production farms.
- 1 dose of live vaccine plus one dose of inactivated vaccine before transfer to production farms.
In this type of vaccination programme, success or failure depends on a programme that meets the key points specified at the beginning of this article.
Conclusions
The reasons for using aMPV vaccines have gained strength in the last few years based on the following:
- Prevention of disease-related mortality, clinical symptoms and economic losses
- Improvement in end product (eggs or chickens) quality
- Rational use of antibiotics.
The control of avian metapneumovirus is not too complex, providing that control programmes are supported by correct diagnosis, vaccination programmes and monitoring. The inclusion of live vaccines against aMPV such as HIPRAVIAR® SHS, in response to an emergent problem in broier chickens, has increased knowledge of the disease and the need for information about its method of action and vaccination strategies.
In long cycle birds such as breeders, most veterinarians are familiar with the disease and how to use the products available on the market. In commercial layers, however, the use of products such as HIPRAVIAR® SHS or HIPRAVIAR® TRT varies from one region to another, and poor diagnosis or the use of antibiotics without establishing the real cause lead to inadequate control of the disease.
In many countries with considerable industrial production, we see how the disease is a growing concern and so is starting to be controlled, first in turkeys, then in breeders and finally in layers and meat production.
HIPRA provides the tools required to support the poultry industry, from diagnosis to control, with a wide range of products to tackle aMPV.

