







Fowl Pox in Layers: An Overview
Fowl pox is a common and economically important disease of layers, causing drops in egg production and increased mortality. 2 August 2016
2 August 2016
 8 minute read
8 minute read
 By:
By: The disease is a slow-spreading one, characterised by the development of skin lesions on the unfeathered skin of the head, neck, legs and feet (dry pox).
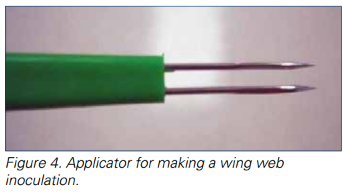
The diptheritic (wet pox) lesions are associated with the upper digestive and respiratory tracts, especially the larynx and trachea. Wet pox is the more serious form of the disease, with higher mortality in flocks.
Wet pox alone can cause high mortality of up to 50–60 per cent in unvaccinated flocks. In layers, the disease causes a drop in egg production and reduces growth and development in young chicks and pullets.
Etiology
Pox viruses have been observed in many avian species with worldwide distribution; however, they tend to be species-specific.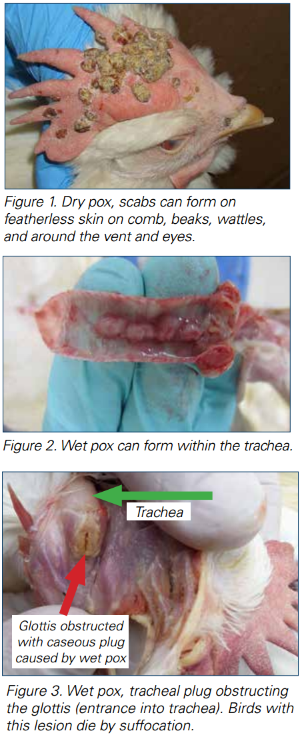
The term “fowl pox” initially included all pox virus infections of birds, but now it primarily refers to the disease of chickens.
All ages are susceptible to fowl pox infection except recently hatched chicks, but the incidence is variable among flocks, dependent on management systems. In high-density, multiple-age farms, the disease may persist for long periods of time despite preventive vaccinations.
Transmission
The virus-containing crusts (scabs) from skin lesions contaminate the environment and facilitate mechanical transmission of the virus between birds.
The virus persists in the environment and may later infect susceptible birds by entering the skin through minor abrasions. In a contaminated house, the aerosol generated by feathers and dry scabs containing pox virus particles provide suitable conditions for both skin and respiratory infection.
Inhalation or ingestion of virus, or virus-infected cells shed from skin lesions, can lead to the diptheritic (wet) form of the disease.
The infection spreads easily from bird to bird, cage to cage, and through ingestion of standing water in drinkers. Insects can serve as mechanical vectors of pox viruses, spreading infection by depositing virus in the eyes of birds or by biting birds.
Crews handling birds may carry the virus on their hands, clothing and equipment, and may transmit the virus to birds through the eyes or skin. Fowl pox vaccine spilled inside the house during vaccination can produce pox lesions on exposed birds.
The mucous membranes of the trachea and mouth are highly susceptible to the virus, and infection may occur in the absence of apparent injury or trauma.
Incubation period
The incubation period varies from about 4-10 days in chickens. Pox spreads slowly within a flock. In cage operations, the outbreak may occur in one section of the house.
Clinical signs and lesions
The disease may occur in either one form (dry or wet pox), or both forms. Clinical signs can vary, depending on the susceptibility of the host, virulence of the pox virus, distribution of lesions, and/or other complicating factors.
Dry Pox:
- Predominates in most outbreaks
- Proliferative nodules (scabs) on unfeathered skin areas of head, neck, legs and feet
- Skin lesions vary in appearance, depending on the stage observed – papule, vesicle, pustule or crust (scab)
- Progression of pox lesions:
– Papules: the initial lesions, light-colored nodules in skin
– Vesicles and pustules: raised yellow lesions
– Crust (scab): the end-stage lesions, reddish brown-to-black lesions
- Cutaneous eye and mouth lesions interfere with the bird’s ability to eat and drink
- Birds lack vigor and have loss of appetite and reduced egg production
- Low mortality if uncomplicated disease.
Wet Pox:
- Cankers or diptheritic yellowish lesions occur on mucous membranes of mouth, esophagus or trachea
- Lesions in the nasal cavity or conjunctiva of eye lead to nasal or ocular discharge
- Reddened (hemorrhagic) tracheas
- Thickened tracheal wall with proliferative and inflamed lesions on the interior surface
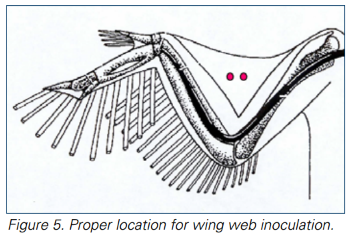
- Lesions can interfere with eating, drinking and breathing; wet pox involving the trachea can result in high mortality due to impairment of breathing
- Unthriftiness and reduced egg production
- Mortality due to suffocation, starvation and dehydration
- Mild to severe respiratory signs; birds typically die due to obstruction of trachea at the glottis
- Respiratory lesions and clinical signs can be very similar to infectious laryngotracheitis (ILT).
- Other differentials are viscerotropic velogenic Newcastle disease (vvND), avian influenza (AI), Mycoplasma gallisepticum (MG), infectious coryza, and fowl cholera.
Diagnosis
Although both dry and wet pox lesions are quite characteristic and their visual appearance may be enough for a presumptive diagnosis, it is possible for dry pox lesions to resemble scabs from other types of trauma to the skin, and wet pox lesions can resemble laryngotracheitis (ILT) lesions in the trachea.
Therefore, a diagnosis of pox should be confirmed with histopathology of the lesions. The presence of intracytoplasmic inclusion bodies is diagnostic for pox virus infection.
Treatment
There is no satisfactory treatment for fowl pox infection.
Intervention strategies
Management procedures
- Cleaning/disinfection of the environment
- Dust control
- Effective insect control programme
- Biosecurity programme to prevent movement of outside contaminated personnel and equipment from entering chicken houses.
- Crews used for vaccination, beak trimming and transfer are a common way the infection is carried between flocks
- Iodine disinfectant added to the water in the face of a fowl pox outbreak can aid in reducing mortality and slowing the spread of infections. – 4-6 oz. iodine/gal (30–50 ml/L) stock solution, metered at 1 oz./gal (7.8 ml/L) of drinking water
- Control cannibalism with proper beak trimming and reduced environmental light intensity.
Variant strains of fowl pox
In some parts of the world, new fowl pox “variant” strains have emerged due to the integration of various genome segments of reticuloendotheliosis virus (REV) into the pox genome. This results in the new virus being more difficult to control with standard fowl pox vaccines.
Affected flocks will typically test positive for REV antibody, but do not have tumours or other signs of REV infection. New vaccines may be developed to better control these pox strains in the future.
Anecdotal evidence suggests that use of a mix of fowl pox plus pigeon pox vaccine may improve protection against these variants.
Vaccination
Where fowl pox is endemic, chickens should be vaccinated to provide protection against fowl pox infection. There are a variety of live, live attenuated and recombinant fowl pox vaccines available on the market. Vaccination should occur prior to expected exposure to the virus.
Chicks can be vaccinated as early as one day of age with a frozen cell/tissue culture origin (TCO) vaccine at hatch in combination with the Marek’s disease vaccine. This early vaccination does not provide long-term pox virus protection for the bird; however, it should provide adequate protection until the second vaccination at 8-10 weeks of age.
For long-term protection, pullets should be vaccinated with a chick embryo origin (CEO) vaccine after 6 weeks of age. These birds are vaccinated by the wing web-stick method using an applicator with two slotted needles dipped in vaccine (Figure 4).
In high challenge areas, pullets may need two vaccinations in the rearing period, at hatch or prior to six weeks of age, and a second at 8-14 weeks of age.
Long incubation period and slow spread of pox infections make it feasible to vaccinate during an outbreak to limit the spread of the disease. Consider vaccinating flocks adjacent to an outbreak, if they are not already vaccinated.
Available fowl pox vaccines
- Fowl pox virus (FPV) vaccine: a CEO (chicken embryo origin) vaccine contains live FPV capable of producing serious disease if applied incorrectly.
- Attenuated FPV vaccines: TCO (tissue culture origin) can be used on chicks as young as one day of age in combination with Marek's vaccines.
- Pigeon pox virus vaccine: a CEO vaccine contains live pigeon pox virus and can be used alone or in combination with the FPV vaccine.
Pigeon pox can administered to birds older than 4 weeks of age. A combination of fowl and pigeon pox vaccines stimulates broader immune response with better overall protection. A full dose of fowl pox and pigeon pox vaccines can be mixed together and given in one application via wing web.
- Live FPV-vectored recombinant commercial vaccines are available (e.g. Newcastle disease-FPV, ILT-FPV).
Live fowl pox vaccine is used as the vector virus to deliver and present vaccine antigens to the host. Potentially improved quality and strength of the immune response generated.
Vaccine "Takes"
Vaccination via the wing web method produces a small lesion, or “take,” which appears post vaccination as a swelling of the skin or small scab at the site of vaccination. This tissue swelling is the best evidence of a successful pox vaccination.
In large flocks, about 10 per cent of the flock should be examined for "takes" approximately 5–6 days post-vaccination.
Out of the examined pullets, 99–100 per cent of those birds should have "takes" present. A lack of the proper amount of "takes" can result from: (1) application to an immune bird, (2) lack of potency of vaccine (e.g. used after expiration date or vaccine exposed to deleterious effects), or (3) improper application.
Many pox outbreaks are a result of improperly administered vaccine
Live pox virus vaccines should be used within one hour of preparation and should not be exposed to conditions that could inactivate the virus. It is important to evaluate pox vaccination crews and correct application problems..PNG)
Crew assessment sheets should include flock identification, cage row number/level, vaccinator’s name, and both start/finish date and times. The quantity of vaccine used per flock should also be checked and recorded.
In flocks that receive multiple pox vaccinations or one at a day of age, the percentage of "takes" or degree of vaccine reaction from subsequent vaccinations will be lower than 99–100 per cent, due to protection from an earlier vaccination.
"Takes" should still be checked and recorded after each vaccination event in order to develop a complete flock history.
Diagnostic re-vaccination with fowl pox vaccine
Checking post-vaccination "takes" is the best method of checking immunity. Another method is to select 200–300 birds in a flock at 18–20 weeks of age that have received a pox vaccine and to re-vaccinate them with a full dose of fowl pox vaccine.
These birds should be checked for "takes" 5–6 days post-vaccination, and 99-100 per cent of those birds should not have "takes."
A "take" at this time means that these birds did not have protection from the earlier vaccination and were susceptible to field challenge. Flocks at this age (before production) may be susceptible to severe pox challenge that do not show at least 95 per cent protection and may require re-vaccination.

