Chicken Health and Dietary Patterns
An extract from a report entitled 'Food, Health and Nutrition: Where Does Chicken Fit?' by the Smart Foods Centre, University of Wollongong and the Animal Research Institute, Department of Primary Industries and Fisheries for Queensland, Australia. 30 May 2008
30 May 2008
 11 minute read
11 minute read
Introduction
As science exposes the fine detail of the food-health relationship, practitioners need information to help guide patients in making healthy food choices. With the exception of breast milk in infancy, no single food provides all the nutritional requirements to sustain and protect the human body. The answer lies in the total diet but achieving a balanced diet requires an ability to discriminate between foods. From a nutritional perspective, this means appreciating the health and disease impacts of dietary patterns, individual foods and specific food components. From a consumer perspective, it also means addressing personal and cultural values, ranging from taste preferences to environmental issues. Moving from an individual to a broader social context brings industry into perspective as the provider of food. This review considers the case of chicken and the health of Australians, and, in moving through the various perspectives, addresses the question: where does chicken fit?
Chicken Health and Dietary Patterns
The links between health and dietary patterns are studied by various means, with intervention studies providing the highest level of evidence for dietary recommendations. Food choice remains at the heart of the research, but the focus can shift from a positive stance (ensuring adequate nutrition) to a negative one (reducing disease risk). Obesity is arguably the most significant food-related health issue for Australians today. Overweight and obesity are major predisposing factors for diseases such as diabetes, hypertension, coronary heart disease and certain forms of cancer. Management of overweight, especially before the development of these complications, is particularly relevant for Australians, with more than half of the adult population and over one-fifth of children aged 5–17 years being overweight or obese.
The Role of Chicken in Healthy Diets
Chicken delivers important nutrients
Lean chicken meat is an excellent source of protein, has a favourable ratio of unsaturated to saturated fatty acids and delivers essential vitamins and minerals. The health impact of chicken is linked to its nutritional composition and the interactions of those nutrients within the food. The nutrient composition of stir-fried chicken breast meat is compared with stir-fried cuts of other meats in Table 1.
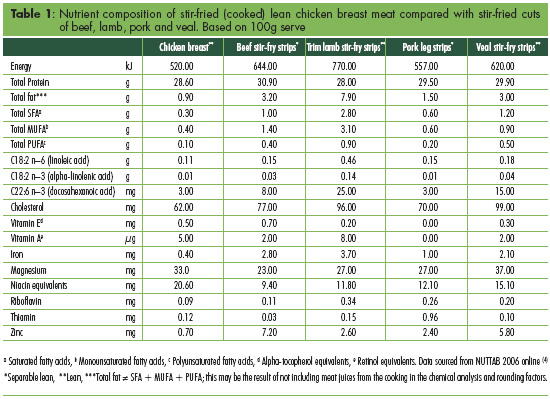
Compared to other meat sources, stir-fried lean chicken breast has the lowest total fat content. The type of fatty acids contributing to this total fat profile should be noted. Stir-fried lean chicken breast contains more than 55% unsaturated fatty acids (monounsaturated and polyunsaturated) and one of the lowest levels of saturated fatty acids when compared with other stir-fried meat sources. Stir-fried chicken breast also appears to be higher in a number of micronutrients although removal of the skin from the meat reduces these figures considerably. Stir-fried lean chicken breast is an excellent source of niacin, providing higher amounts than each of the other lean stir-fry cuts of meat. For other macro- and micro-nutrients, stir-fried lean chicken breast has a similar nutrient profile to lean stir-fried cuts of beef, lamb, pork and veal although it contains relatively little iron and less zinc than the cuts of beef, lamb, pork and veal used in this comparison.
The nutrient profile of chicken meat has been shown to be amenable to manipulation by different feeding practices. For example, dietary supplements such as garlic, copper, omega-3 fatty acids and dehydrated alfalfa have been used in an attempt to change the fat and cholesterol content of poultry meat. It is possible to change the fatty acid profile of chicken meat to increase its omega-3 fatty acid content by feeding chickens either linseed or rapeseed extract (ten-fold increase in alpha-linoleic acid, ALA), or fish extract or algae oils (seven-fold increase in long chain docosahexaenoic acid, DHA).
Such innovations in the production system may further increase the potential benefits of chicken meat in the diet in years to come. The nutrient composition of Australian chicken meat is also affected to some extent by the type (breed) of chicken, butchering technique (for example, the amount of trim), age and sex of the bird.
At present, there appears to be no conclusive body of data demonstrating significant differences between the nutritional composition of conventional, organic, free-range and kosher chicken meat.
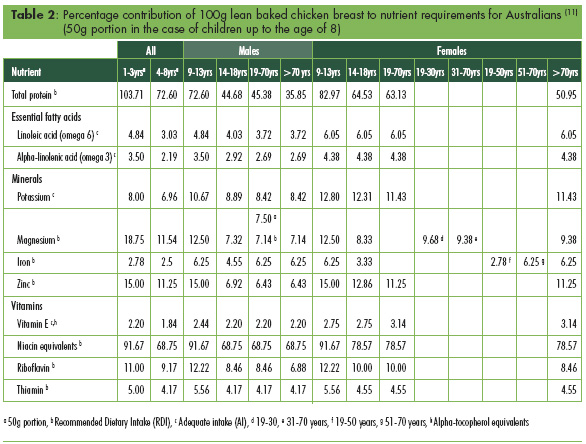
Chicken contributes to nutrient requirements
To establish how chicken can contribute nutritionally to a whole diet, the nutritional values for a serve of chicken meat can be compared with the recommended dietary intakes of Australians. When this was done for all age groups and for both genders, baked lean chicken breast alone was found to provide 68-91% of daily niacin requirements (Table 2). Lean chicken breast was also found to be an important source of protein, providing more than 50% of the recommended dietary intake (RDI) for all ages except 14-18 year old males who have higher protein requirements. For children, lean chicken breast is a good source of magnesium (11.5-18.8%) and zinc (11.3-15.0%), and provides reasonable amounts of riboflavin (9.2-12.2%). Thus, from a nutritional perspective, chicken can fulfil a valuable role in the Australian diet. Lean chicken meat is a good source of protein, and its high protein content may support efforts at weight management. It is also a low-cholesterol meat that contains essential fatty acids and is a source of minerals and essential vitamins, particularly vitamin E, vitamin A and thiamin, and delivers significant amounts of niacin, an important nutrient for energy metabolism.
Weight loss and cardiovascular disease risk factors
High-protein diets have proven effective in weight loss, both in the short and long term, suggesting a role for foods that deliver high quantities of protein, such as chicken.
In one study of 54 postmenopausal women comparing hypocaloric diets of high protein (provided mainly by chicken or beef) and high-carbohydrate diets, a similar reduction in mean energy intake was achieved between the groups over nine weeks.
Here, the chicken diet - but not the beef diet - showed a significantly higher weight and body mass index loss than the high carbohydrate diet (representing losses of 7.9 and 5.6kg, respectively; P<0.05). However, weight loss was not statistically different between the chicken and beef diet groups. These findings were confirmed in a similar 12-week study in which weight loss did not differ according to allocation to a diet where the predominant protein source was either lean beef or chicken. This group concluded that weight loss and improved lipid profile effects were best achieved by high dietary protein regardless of the comparative food source. This position was supported by an earlier study of appetite responses, which found postprandial satiety responses did not differ in meals of beef or chicken in young lean Australian men.
Chicken has a role within the context of a low-fat eating plan in cholesterol-lowering diets. Incorporation of either chicken, lean beef or lean fish in an American Heart Association diet showed that plasma total and LDL cholesterol can be reduced by 7–9% over a short period of time (26 days) in hypercholesterolaemic men, irrespective of the protein source. These findings confirm the findings of earlier research.
Whole dietary models are also of interest in determining the position of individual foods in protecting cardiovascular health. The DASH diet, for example, has been shown to be effective in lowering blood pressure, particularly in people with hypertension and in African Americans. This diet emphasises chicken and fish, and includes nuts and low-fat dairy products, alongside high proportions of fruits and vegetables.
From a more general perspective, further information on the position of individual foods can be considered in terms of other dietary relationships. In a large US cross-sectional survey of children (n=4,802) and adults (n=9,460), for example, the inclusion of an average intake of less than 28g of chicken over two days was associated with lower discretionary fat intakes compared to non-consumers or consumers of larger portions (≥28g cooked lean chicken equivalent per two days; P<0.05). This highlights the importance of portion size, a key component of guidance on food choice.
Chicken and cancer risk
In 2007, the World Cancer Research Fund (WCRF) published a recommendation that intake of red meat (beef, pork, lamb and goat) should be limited, and in those who consume red meat, less than 500g a week is the dietary target. WCRF also recommended that processed meats should be avoided. Links between diet and cancer are difficult to ascertain because by nature, there is a reliance on associations reported in observational studies. The WCRF report determined that the evidence was too limited in amount, consistency or quality to draw any conclusions regarding poultry consumption and cancer risk. A brief indication of why this is the case can be seen from a summary of published studies (accessed on PubMed) in the period 1996-2007.
Of seven papers identified in a systematic search on colorectal cancer risk, five found a protective association with increased chicken consumption, one found no association, while another found a positive association between cooking method for chicken (i.e. preferring darkly browned surfaces) and cancer risk. For breast cancer, increased chicken consumption was either associated with no additional risk or was found to be protective, regardless of cooking method. One case-control study found that postmenopausal women with oestrogen receptor-positive tumours were more likely to consume a dietary pattern that included chicken, along with other foods, than controls without cancer. For bladder cancer, an increased risk was associated with skinless chicken consumption of more than five times per week, but this was not found for chicken consumed with skin. It was hypothesised that chicken without skin contains more heterocyclic amines than chicken cooked with skin. A large prospective cohort study (n=110,792) from Japan found a significant inverse association between hepatocellular mortality and chicken consumption in men, and another case-control study from China also reported protective effects of chicken consumption on hepatocellular cancer risk. Two studies on gastric cancer found either a decreased mortality risk associated with chicken intake or no association between chicken intake, including cooking method, and risk of adenocarcinoma of the stomach and oesophagus. No association has been shown in a study investigating chicken consumption and ovarian cancer risk.
Despite a number of studies suggesting some protective effects of chicken meat against cancer, the overall evidence is not conclusive.
There is emerging evidence that the cooking method of meat is possibly more important than frequency of consumption of specific foods in determining risk of various cancers. In a study of pancreatic cancer risk, more cases than controls showed a preference to well-done meats, including bacon, grilled and pan-fried chicken. Similarly, Norrish and colleagues reported a weak and inconsistent association between meat doneness and increased risk of prostate cancer but this was not significant for chicken. Thus while there is no conclusive evidence linking chicken meat with cancer or its prevention, cooking methods that generate carcinogenic compounds such as heterocyclic amines (HCA) and polycyclic hydrocarbons (produced when meats are cooked over an open flame or charred) deserve some attention. Reduced levels of HCA have been found in chicken that has been marinated before grilling. Meats (beef patties) that are partially cooked in a microwave oven before being cooked by higher temperature methods also have lower levels of these compounds. A review by Thomson reported that the most important variables contributing to HCA formation are: cooking temperature (>150ºC), cooking time (>2 min), cooking method (frying, oven grilling/ broiling, barbecuing) and meat type. However, much of the evidence relating to the formation of HCAs and polycyclic hydrocarbons in various meats prepared using different cooking methods is inconsistent and reported absolute amounts of these compounds are highly variable between studies. Undoubtedly, further well-controlled studies are required to inform consumers of the best way to prepare meat in order to minimise health risks.
Food Safety is an Important Consideration
Safe food handling is a concern for all foods. From 1995 through 2000, 214 outbreaks of food-borne disease were identified in Australia, affecting a total of 8,124 people. Seventy-four of these outbreaks, involving 6,472 people, had a known aetiology. Bacterial disease was responsible for 61% of the outbreaks, with salmonella being the most common pathogen (35% of outbreaks), followed by Clostridium perfringens (14%), ciguatera toxin (11%), scombrotoxin (3%) and norovirus (3%). There were 20 deaths attributed to food borne illness; salmonellosis and listeriosis were each responsible for eight (40%) of the deaths. Restaurants and commercial caterers were associated with the highest number of outbreak reports and cases, followed by hospitals and aged care facilities. The most frequently implicated vehicles in the 173 outbreaks with known vehicles were meats (30%), fish (16%), seafood (6%), salad (6%), sandwiches (5%) and eggs (4%). Chicken, the most frequently implicated meat, was associated with 27 (13%) of the outbreaks.
Food safety risks can be minimised by following some basic storage, preparation and cooking practices as bacteria can become a problem if food is not stored and handled correctly. Chicken meat is a perishable food and therefore should not be kept at room temperature for more than two hours. Raw meats should be stored at a maximum temperature of 4ºC or kept frozen below -15ºC. Frozen chicken meat should always be thawed completely prior to cooking. Separate utensils should be used in preparation and cooking should ensure 75ºC at the centre of the thickest part of the meat, producing clear juice at the end. Stuffing should be inserted loosely before, and removed immediately after cooking. Chicken that is to be kept hot should be kept above 60ºC and leftovers should be stored in the fridge for one to two days only or be frozen. Leftovers should be heated to at least 70ºC for a minimum of two minutes. Although listeriosis is not rated a significant risk from chicken meat, in pregnancy chicken is best consumed hot immediately after cooking, and any leftovers stored in the fridge and used within a day of cooking or purchase.
Further Reading
| - | You can view the full report by clicking here. |
May 2008